Соматотропный гормон (соматотропин, гормон роста) - это один из тропных гормонов передней доли гипофиза. Соматотропный гормон пептид, который как и другие гормоны переносится кровью к определенным органам-мишеням и оказывают на них специфическое, не воспроизводимое никакими другими веществами, действие. Это действие по своему механизму представляет собой стимуляцию или угнетение каталитической функции некоторых ферментов в клетках органов-мишеней. Таким образом, соматотропный гормон сам не является субстратом химических процессов, на которые он влияет. Он лишь является носителем управляющей информации и в функциональном отношении сравним с сериями управляющих нервных импульсов. Посредством соматотропного гормона нервная система осуществляет следующие функции: (а) Управляет физическим, половым и умственным развитием организма; (б) Управляет активностью всех систем организма, ее соответствием актуальным и потенциальным потребностяморганизма в меняющихся условиях среды (адаптация). (в) Регулирует (поддерживает устойчивость) уровень ряда физических переменных, таких как осмотическое давление, pHжидких сред организма, концентрация глюкозы плазмы крови и т.д. (гомеостаз). С функциональной точки зрения соматотропный гормон относят к гландотропным (тропным) гормонам. Тропные гормоны - это гормоны, которые влияют на синтез, резервирование и секрецию эффекторных гормонов, гормонов, которые действуют непосредственно на орган-мишень. К ним относятся глюкокортикоиды коры надпочечников, гормоны щитовидной железы, половые гормоны и ряд других гормонов. В свою очередь, процессы синтеза, резервирования и секреции тропных гормонов управляются другой большой группой гормонов - гормонами гипоталамуса. Среди нихрилизинг-гормоны (активирующие синтез, секрецию и высвобождение гормонов гипофиза) и ингибирующие (тормозящие синтез, секрецию и высвобождение гормонов гипофиза) гормоны, через которые нервная система передает свои влияния по цепи гормональных исполнительных механизмов к различным объектам управления.
Гипотетические механизмы гормонального управления процессами роста
Предполагается существование трех возможных механизмов гормонального управления процессами роста. В соответствии с первой гипотезой гормон роста (growth hormone, GH) стимулирует выработку инсулиноподобного фактора роста-1 (соматомедин, insulin-like growth factor 1, IGF-1). Повышение концентрации соматомедина в циркулирующей крови(эндокринный соматомедин) действует на эпифизеальную пластинку (пластинка роста, гиалиновая пластинка хряща в метафизах длинных костей). В соответствии со второй гипотезой гормон роста регулирует выработку клетками печени: (а) связанного с белком соматомедина-3 (IGF-binding protein 3, IGFBP-3) и кислотно-лабильных субъединиц (acid-labile subunit, ALS) комплекса белок-соматомедин (IGFBP complex). Соматомедин связывается с кислотно-лабильными субъединицами комплекса белок-соматомедин. При этом образуется трёхкомпонентные комплексы (150-kd ternary complex). В последующем протеазы расщепляют эти комплексы на фрагменты, высвобождающие в гемациркуляторное русло связанный с белком соматомедин-3 и инсулиноподобноый фактор роста-1, действующие на эпифизеальную пластинку. В соответствии со третьей гипотезой гормон роста вызывает дифференцирование и местную выработку инсулиноподобного фактора роста-1 (соматомедин). По паракринному и аутокринному механизму соматомедин стимулирует деление клеток.T3, triiodothyronine = трииодтиронин. Последовательность реакций, вызванных гормоном роста. Взаимодействие гормона роста с соматомедином
GH, growth hormone = гормон роста; GHBP, GH-binding protein = циркулирующий с кровью гормон роста, связанный транспортным белком; GHRH, growth hormone-releasing hormone = соматолиберин; IGF-1, insulin-like growth factor 1, also called somatomedin C = инсулиноподобный фактор роста-1, или то же что соматомедин - биоактивный белок печени и мышц, посредник гормона роста. IGFR, IGF-1 receptor = рецептор соматомедина (инсулиноподобный фактор роста-1); FFA, free fatty acids = свободные жирные кислоты; SRIF, somatostatin = соматостатин. Отношения гипоталамуса и гипофиза в управлении секрецией гормона роста
Секреция гормона роста (GH, growth hormone) гипофизом активируется соматолиберином (GH-releasing hormone, GHRH) и тормозится соматостатином (somatostatin, SRIF). На уровне гипофиза существует управление секрецией гормона роста посредством инсулиноподобного фактора роста-1 (insulin-like growth factor I, IGF-I) и посредством свободных жирных кислот (free fatty acids, FFA). Гормон роста также активирует нейроны (SRIF neurons) перивентрикулярного ядра гипоталамуса, секретирующих соматостатин. Таким образом реализуется механизм короткой отрицательной обратной связи в управлении секрецией гормона роста. Аксоны нейронов, секретирующих соматостатин, заканчиваются синапсами на нейронах (GHRH neurons) дугообразного ядра, вырабатывающих соматолиберин и посылающих свои аксоны к срединному возвышению гипоталамуса. Нейроны дугообразного ядра также непосредственно модулируют секрецию гормона роста по интегрированным сигналампериферического гормона роста, лептина и грелина. Эти нейроны дугообразного ядра, вырабатывают нейропептид-Y (neuropeptide Y, NPY neurons) и реализуют его к перивентрикулярным нейронам (periventricular SRIF neurons), секретирующим соматолиберин. Грелин секретируется в желудке и является гипофизарным естественным лигандом для биохимических рецепторов, участвующих в активации секреции гормона роста, как на гипоталамическом, так и на гипофизарном уровне. Установлено, что выведение соматолиберина активируется галанином, γ-аминомасляной кислотой (γ-aminobutyric acid, GABA), иα-2-адренергическими и дофаминергическими (DA, dopamine) сигналами, но тормозится соматостатином. Секреция соматостатина тормозится ацетилхолином (ACh, acetylcholine, мускариновые рецепторы) и 5-гидрокситриптамином (серотонин,5-HT, 5-hydroxytryptamine, рецепторы типа-1D). Секреция соматостатина активируется α-2-адренергическими сигналами и кортиколиберином.
Hormones are the chemicals produced within the body by some specialized cells and have specific effects on the activity of target organs through specific receptors. There are 2 types of hormones:
eg. All other hormones except steroid and thyroid hormones
Before Moving on to the mechanism of action, we will list the major steroid and thyroid hormones.
Steroid hormones (Cholesterol derivatives):
Glucocorticoid (Cortisol)
Estrogen
Testosterone
Progesterone
Aldosterone
Vitamin D (Calcitriol)
Thyroid hormones (Amine derivatives):
Tri-iodothyronine (T3)
Thyroxine (T4)
Mechanism of Action of Steroid Hormones:
Simple Diffusion: The lipid soluble hormones diffuses through the cell membrane to enter the cell.
Hormone binds to the intracellular receptor composed of a "Hormone binding" domain, a "DNA binding" domain and a "amino terminal" which interacts with other transcription factors. Binding of the hormone leads to exposure of DNA binding zone.
Hormone-receptor complex enters nucleus and dimerizes.
Binding to HREs: Hormone-recpetor dimers bind to Hormone (Steroid) Receptor Elements (SREs or HREs) of DNA.
Transcription: DNA transcription leads to formation of mRNA.
Translation: mRNA undergoes translation to produce new proteins. e.g. Calbindin for Vitamin D
Physiologic action of hormones.
What is the difference in the mechanism of action of thyroid and steroid hormones?
After passing through the cell membrane, steroid hormones except calcitriol bind to the intracellular receptor in the cytosol before entering the nucleus while the thyroid hormones and calcitriol directly enter the nucleus to bind to the intranuclear receptor. Beside, this difference all other steps are similar for both the hormones.
Steroids are a very taboo subject in our culture. They are Schedule III controlled substances, meaning they are illegal to own without a prescription, and illegal to distribute unless you are an MD. Furthermore, they are banned in almost all athletic competitions (with the exceptions being some untested strength sports). This is not meant to be read as an article condoning steroid use. They carry numerous short-term risks (high blood pressure, high cholesterol, liver toxicity, etc.), with the potential for long-term risks (atherosclerosis, infertility, hypogonadism, etc.) dependent on the particular compounds used, the dosages, and the duration you take them. Anyone who knows anything about steroids has probably heard about the risks they carry, so I’m not going to beat you over the head with that.
With that standard disclaimer out of the way, I still think steroids are worth having frank, open discussions about, for two main reasons.
They’re really interesting.
People are going to use anyway, so they may as well be informed.
In fact, as of 2002, 4% of high school students were willing to self-report that they had used steroids, and that number was trending upwards. If I had to take a guess, that number is probably low since people are known to underreport their involvement in socially undesirable behavior, even if they know they’ll remain anonymous.
Other surveys indicate that between 1-3 million Americans use steroids. For context, there are about 60 million people with gym memberships in the country, and 2/3 of those people never go to the gym, taking the number of actual gym goers down to about 20 million. If we assume that the people using steroids are actually working out, that means that between 1 in 20 and 1 in 6 people you see in the gym are on, or have at least tried, steroids. It’s hard to pin down an exact number because these types of surveys about illegal behavior are notoriously unreliable, but it’s safe to say that it’s certainly a not a negligible proportion of the gym going population.
Odds are, whether they’re open about it or not, you know someone on steroids.
(If you’re interested in understanding the basic physiology of how steroids work, then just keep reading from here. If you already know it, or if it doesn’t interest you, skip ahead a couple pages to the subheading “Steroids work, in part, because you expect them to work.”)
The first question is, how do they work?
The mechanism of action for steroid hormones (like the anabolic steroids we’re talking about, though the same is true of any steroid hormone including cortisol, estrogen, aldosterone, etc.) is pretty straightforward. They’re lipid-soluble, so they can diffuse directly into a cell (rather than needing to bind to an receptor on the surface of the cell like peptide hormones – like insulin and IGF-1), bind to their particular steroid receptor, and go to the nucleus of the cell so they can influence gene transcription. Those transcribed genes determine what proteins are produced, and those proteins affect the structure and function of that cell.
from tube.medchrome.com
The steroids we’re talking about are mostly derivatives of testosterone (or similar hormones like DHT, though some like Deca-Durabolin are derivatives of progesterone), and have the same mechanism of action. They diffuse into the cell, bind to a receptor, influence gene transcription, and ultimately influence the proteins the cell produces. Different steroid hormones cause cells to produce different proteins, but in skeletal muscle, testosterone and its derivatives primarily increase the production of the actin and myosin that are the major proteins that make you strong and jacked.
Backing up a step, though, before these steroids can make their way into the muscle to have an effect, they have to actually travel in the blood to the muscle.
So the first issue is getting those steroids into your blood. Routes of administration that don’t involve digestion tend to be the safest for your liver, including injections and transdermal administration (like Androgel). Oral steroids have to be modified so your liver can’t immediately excrete them – things you swallow are absorbed, and then pass through your liver before they can make it to general circulation. Your liver isn’t particularly keen to pass high doses of steroid hormones directly to general circulation, so it will break them down into non-bioactive metabolites unless they’re modified to resist this process. Because of this, your liver tends to have to work quite a bit harder to handle orals than injectables, so orals tend to be more damaging to your liver. There are orals that aren’t very hepatotoxic (damaging to your liver), and there are injectables that are quite hepatotoxic, but since this post isn’t meant to be a how-to guide for steroid use, recognize I’m painting in broad strokes here.
Now that the steroids are in your blood (either by direct injection, or because they survived their first pass through the liver), they need to make it to your muscles.
Most testosterone in your body is bound to proteins in your blood, most notably albumin and sex hormone binding globulin (SHBG). If you get your testosterone levels checked, the lab should report total testosterone, and free testosterone. The free testosterone is the stuff that’s most available to diffuse into your cells and affect the body.
This is a key point, and is the main reason why steroids don’t seem to have much effect until they’re taken in supraphysiological doses – presenting your body with a concentration it wouldn’t experience in normal circumstances. When you don’t have any major endocrine problems and your testosterone levels are within the normal physiological range, your body will produce more or less binding proteins to make sure you have the right amount of free testosterone – not too little, and not too much.
Your body can’t just jack up albumin production because it plays a critical role in keeping fluid concentrations stable between your cells and the extracellular fluid, and while SHBG levels increase when you introduce high levels of some exogenous steroid hormones into the body (including estrogen, which is a major reason many women experience loss of sex drive when they go on birth control – increased SHBG binds more of their precious, tiny amounts of testosterone that are so important for sex drive), testosterone actually decreases SHBG levels slightly for reasons I admittedly don’t quite understand.
This is the main reason why over-the-counter “testosterone boosters” don’t work for building mass and strength if you have normal testosterone levels, and steroids work really really well. Even if your test booster increases your testosterone by 40% like it claims, you’re still relying on your testes to produce it, and they simply won’t pump out enough to push you to supraphysiological concentrations to outrun the effects of the binding proteins. You could have 40% more testosterone but the same free testosterone.
So, this was a long way of explaining why steroids “work.” You put enough of a hormone into the body that the body’s normal regulatory mechanisms can’t quite cope, so you wind up with more free androgens to make it to your muscles and make you jacked.
This is quite a bit more dry physiology than I like going into, but I think it’s important to cover because a lot of people are ignorant of it, and it can help provide a basic backdrop of understanding for discussions about steroids.
Of course, an article basically saying “steroids make you strong, and here’s the physiology behind steroids work,” really wouldn’t be saying much that’s relevant to you. So now it’s time to actually delve into the fun stuff.
Steroids work, in part, because you expect them to work
Let’s take a look at two studies examining the placebo effect’s impact on “steroid-induced” strength gains.
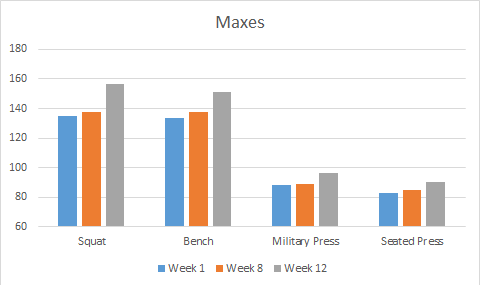
In the first (Ariel, 1974), researchers told 15 trained athletes they could get their hands on some free, legal steroids. The subjects were already relatively strong at the start of the study – with squat and bench press maxes around 300 pounds, and military press maxes a shade under 200 pounds.
They trained for 7 weeks with the promise that the people who made the best strength gains (to give them an incentive to train hard and make as much progress as possible) in those 7 weeks would get free, legal steroids. So the athletes trained for 7 weeks, and put a combined total of ~22 pounds on their bench, military press, seated press, and squat.
Then, 6 of the participants were selected at random to take part in the “steroid” trial. They were told they were being given 10mg/day of Dianabol, when really they were taking placebo pills.
They trained for another 4 weeks, thinking they were on drugs.
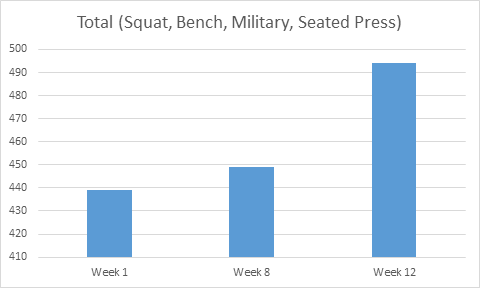
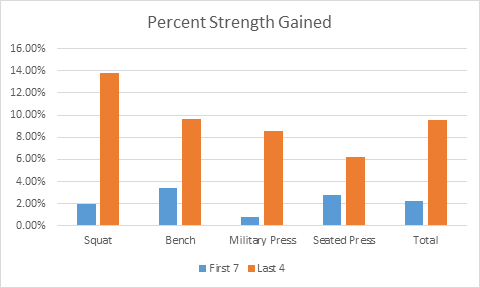
In just 4 weeks, they put a combined total of ~100 pounds on those same four lifts. 100 pounds instead of 22, in 4 weeks instead of 7. Simply because they THOUGHT they were on steroids.
Strength on each lift, in kgStrength on the 4 lifts combined, in kg4x the strength gains in a bit more than half the time. The placebo effect at work, because the lifters *expected* to gain so much strength.
So the placebo effect clearly increases your strength gains from training when you simply *think* you’re on steroids. You expect more gains, so you get more gains.
In this one, the researchers were in a perfect position to study the placebo effect. The researchers were coaching a powerlifting team, and the eleven members of the team actually asked their coaches about using steroids. Presumably they trusted their coaches, so when their coaches told the lifters they were providing them with fast-acting steroids, the lifters bought it hook, line, and sinker.
Their coaches gave them saccharine pills, telling them they were steroids. Then they maxed out on squat, bench, and deadlift.
An important thing to note is that these were all nationally ranked powerlifters. The average bodyweight was around 85kg, with average maxes of 257kg squat, 207kg bench, and 260kg deadlift (566 squat, 456 bench, 573 deadlift at ~187 pounds). Based on how close the bench is to the squat and deadlift, I’m assuming they were lifting in powerlifting gear, but I’m not positive. However, they weren’t new lifters –these guys were really strong.
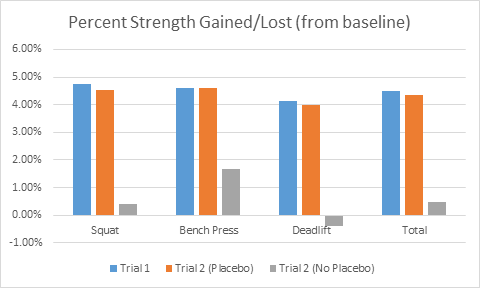
When they maxed, thinking they were on steroids, every single one of them hit PRs on every lift. The smallest PR on any lift was 5kg. Most were 10 or 12.5kg PRs. These PRs represented 4-5% improvements on their maxes, taking their 724kg average total to ~755kg (1597 pounds to ~1670).
After that, they trained for two more weeks, continuing to think they were on steroids.
After these two weeks of training, they were asked how their training had been going. All of them reported that they’d been lifting heavier weights, lifting the same weights for more reps, and generally feeling more energetic and having better training sessions.
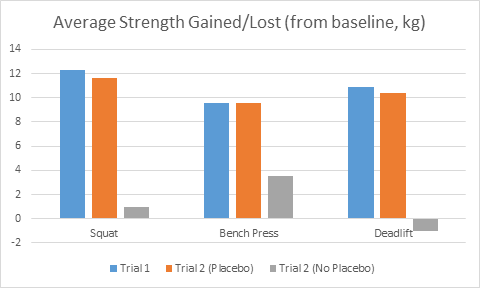
Then they maxed again. However, the coaches put a twist on it. 6 of the lifters were allowed to continue believing they were on steroids. 5, however, were told they had been taking a placebo the whole time.
The results were astounding.
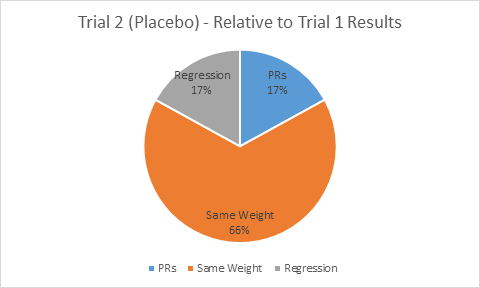
The group that continued to believe they were on steroids stayed at about the same level they had reached two weeks prior. There were a few small regressions and a few small new PRs, but on the whole they held onto the 4-5% extra strength they’d gained by thinking they were on steroids.
The group that was informed they’d been taking a placebo absolutely tanked. Their maxes essentially returned to their pre-placebo baseline. None of them could hit a single lift that equaled what they’d done two weeks prior. This is IN SPITE OF knowing they hadn’t been taking steroids when they had hit PRs two weeks before, and in spite of reporting better training for the two intervening weeks. As soon as the mental crutch was removed, they couldn’t perform on the same level, even though they knew the initial PRs and the two good weeks of training were just the result of their hard work – not drugs.
10-12kg PRs are nothing to scoff at. But notice the gray bars – when they found out they weren’t actually on steroids, their lifts headed back to pre-placebo baseline immediately.4-5% stronger on every lift. When they continued thinking they were on steroids, they kept it. When they didn’t is evaporated, even though they reported two exceptionally good weeks of training, and knew they were drug-free for trial 1 as well.Placebos = PRs all around. 33 opportunities for PRs (11 lifters, with 3 lifts apiece), and 33 PRs, ranging from 5-15kg.Still thinking they were on steroids, there were some 2.5kg PRs and 2.5kg regressions, but most people had just about the same strength as for trial 1.Take the placebo away, and no one could match what they’d done previously, even though they knew they were clean for trial 1, and for two awesome weeks of training in between trials.
So from these two studies we see a piece of why steroids are so effective. On top of how well they work physiologically, when people go on steroids, they THINK they’re going to get a ton stronger. They can lift more weight just by thinking they’re on, and they’ll gain more strength from training just by thinking they’re on. Part of the reason steroids work so well is that you expect them to work so well.
Of course, the effects of steroids aren’t just all in your head. They do, very much, work.
Let’s take a look at a major study (Bashin, 1996) that confirmed what bodybuilders had known for years – namely that supraphysiological doses of testosterone work really really well for building size and strength.
The subjects were split into 4 groups. One group was given a placebo (sesame seed oil injection instead of a testosterone injection) and didn’t lift. One group was given testosterone and didn’t lift. One group was given a placebo and lifted. The last group was given testosterone and lifted.
They maxed on bench press and squat at the beginning and end of the 10 week program. The program itself was a mix of DUP and linear progression, by the sound of it – pretty decent programming if you’re trying to get people bigger and stronger.
The results:
Check out the strength and mass gained while not touching a single weight in the second column. From the New England Journal of Medicine
Yes, you’re reading that chart correctly. The group that took a placebo and worked out only gained slightlymore strength than the group that took testosterone and sat on the couch for 10 weeks. The group that took testosterone without exercise gained just as much, if not more, muscle mass than the people taking a placebo and actually working out.
Keep in mind, the dose for this study was 600mg/week of testosterone with nothing else added in. This wasn’t a several-grams-per-week pro bodybuilder steroid stack. This was a fairly low dose that might represent someone sticking their pinky toe into the world of steroids.
So for people who say, “oh, steroids don’t make you bigger and stronger. They just let you work harder,” I’m sad to inform you that such a statement is patently false. They may help with recovery and let you work harder, but I guarantee you that you could stick with the exact training routine you have now, start taking steroids, and gain more size and strength from it – no extra work required. And an untrained person might (would probably) gain more muscle from just taking steroids than they would if they actually worked out.
Steroids clearly make you bigger and stronger. But how much of an advantage do they actually provide for sports?
For sports where absolute strength and size are paramount, they give a huge advantage: The superheavyweight class of any sport where you can weigh as much as you want comes to mind. Powerlifters, weightlifters, and strongmen in the very top weight division. Obviously bodybuilding and physique sports as well.
For everything else – I think they help, but not to the degree people would like to make it seem, and not at super high doses.
Most sports, at their core, are about producing as much force as possible relative to your bodyweight, while effectively meeting the energetic demands of the sport. The “relative to your bodyweight” piece is the part I’d like to hone in on.
You see, steroids don’t directly make you stronger. They directly make you bigger. They cause your muscles to synthesize more protein, but there’s more to strength than muscle protein accretion. There is a relationship between “bigger” and “stronger” (obviously), but the relationship isn’t 1 to 1.
(edit: the statement “they don’t directly make you stronger” may not be entirely true. Testosterone does have nervous system effects that could directly improve strength output, and many lifters report substantial acute benefits of various fast-acting oral compounds due to mood alteration and lowering of central inhibition. However, the former works on a slightly longer time scale compared to muscle protein synthesis, and the latter DOES probably contribute, but there’s no research to determine how effective orals are at altering mood, perception, and expectancy relative to placebos. Thanks to Dr. Mike Israetel for the catch.)
Especially in sports with weight classes, added muscle mass isn’t good for much if your strength doesn’t increase at the same rate. At least based on the scant research available, it looks like it may be the case that if you take too high of a dose, it’ll actually hinder your performance by increasing your mass much more than your strength.
The first place I’d like to look is at a study examining the effects of different doses of testosterone. Participants’ natural testosterone production was slowed down, and then they were given test in doses ranging from 25mg/week (really really low) to 600mg/week (well above the physiological range).
Linear increase in muscle mass gains, but not much of a difference between 300mg/week (which took the people about 40% above the top of the physiological range) and 600mg/week (which took them several times above the physiological range, effectively increasing their testosterone by 4-5 fold) for strength gains, in spite of the substantially increased mass gains with 600mg/week. From the American Journal of Physiology.
Gain in muscle size was quite linear. However, gains in strength were not. The 300mg/week group got nearly the exact same strength gains as the 600mg/week group, but with less hypertrophy (about 5 pounds less fat free mass). Over time, this could potentially mean lower force output relative to bodyweight for the group taking a higher dose.
This notion is borne out in further research (Yu, 2014), comparing strength and muscle characteristics between lifetime drug free lifters and long-term steroid users. In this study, the steroid users had larger legs and more lean mass, but the drug free lifters squatted considerably more relative to lean body mass and leg muscle volume. Each pound of leg muscle for the drug free lifters could produce more force than a pound of leg muscle for the steroid users.
Check out Maximal Squat Force relative to Lean Leg Mass. 88N/kg vs. 130N/kg – about 47% more force output per unit of muscle for the drug free lifters. From PLoS ONE.
Of course, in this study, a confounding factor is training histories. Due to ethical constraints, there was no intervention – it was merely an observational study. The drug free lifters were all weightlifters or powerlifters, whereas the steroid users included a mix of lifters, strongmen, and bodybuilders. So it could simply be that the differences could be attributable to the sport-specific training, not the drugs. Because the difference was SO profound, though (almost 50% higher force output per pound of leg muscle in the drug free lifters), I don’t think we can chalk it all up to training.
However, I’m not entirely sure WHY someone would be stronger, relatively, if they built their muscle without drugs. Maybe the rapid protein synthesis and decrease in protein breakdown doesn’t allow for effective remodeling. Maybe muscle strength increases faster than tendon strength, so sensory mechanisms like the golgi tendon organ don’t allow the muscles to contract maximally. Maybe the muscle is being built so fast that neural factors simply can’t keep up, so the lifters in these studies wind up with large, inefficient muscles that could be made more efficient with training and by transitioning into a training phase focusing on adding strength without any more mass.
Or, of course, I could be entirely wrong. There’s not a lot of research on steroid use in healthy, athletic populations, and there are obvious confounding factors in both of these studies. I will say, though, it matches some of my observations. The guys on drugs who tend to do the best in weight class dominated sports like powerlifting, are the ones who add mass slowly, gradually increasing their doses or sticking with a conservative cycle for a long time instead of aggressively trying to add a lot of mass all at once. Look how long it took for Ed Coan to go from 165 to 242, as an example. Based on what I’ve seen, the guys who get the most out of their drugs – for strength – are the ones who take enough to primarily improve recovery, while gradually add mass over time – not put on 20+ pounds over night. Going back to Bashin, 2001, if you’re a powerlifter, you want the results of the 300mg/week group, not the 600mg/week group.
The last thing I’d like to talk about is how long steroid use benefits you.
The short answer – basically forever.
When your muscles grow, your muscle fibers add new myonuclei – each nucleus can only “manage” a finite amount of real estate in a muscle fiber, so your fibers have to add more as they grow. If you stop training, you may lose muscle size, but those myonuclei stick around for much, much longer. That’s the main reason behind the phenomenon of “muscle memory.” If you take a few months off lifting, you can come back to the gym and get back to your old levels of strength and muscularity pretty quickly, because your body doesn’t have to fuse new myonuclei again. The old ones are still sticking around (unless the muscle fiber itself dies, as could happen with aging or severe injury), so your body just ramps up protein synthesis and voila! It takes you a month or two to gain back the muscle it initially took you years to build, because protein accretion can proceed at a quicker rate than gaining new myonuclei.
The blue lines represent years of hard training. The red line represents a couple weeks or months. From the University of Oslo.
Of course, the application for steroids is pretty obvious. You take steroids, you gain mass, you go off, and those myonuclei are still hanging around, keeping you more jacked than you would have been otherwise.
So, here are some takeaways:
1) Steroids, physiologically, work. This much is not debateable.
2) On top of how well they work physiologically, a major factor is how well they work psychologically – if you do something expecting to get a ton stronger, there’s a good chance you’ll get a ton stronger. This applies to much more than steroids.
3) Steroids do provide a substantial advantage for sports that aren’t governed by weight classes. However, taking too high of a dose right off the bat may actually decrease performance (increased strength and mass, but decreased relative strength), especially in sports with weight classes. If you decide to use steroids, you’ll probably get the best bang for your buck, strength-wise, with very conservative doses initially.
4) If you take steroids and then come off of them, you’ll probably lose some of the size and strength you gained, but you’ll always be at an advantage relative to a lifetime drug-free athlete.